Anterior Cruciate Ligament (ACL) Tears
Anatomy
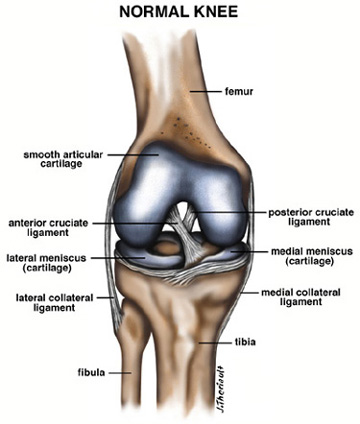
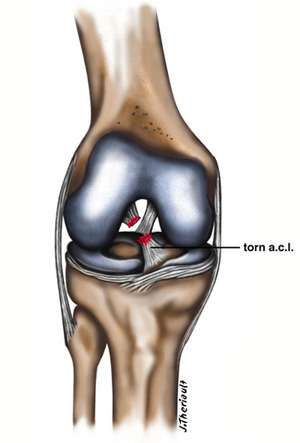
The anterior cruciate ligament is a thick band of tissue which has two major strands that extend from the lower leg bone (tibia) to the thigh bone (femur). This ligament is very important for maintaining stability of the knee. When it is injured or torn the patient feels the instability of the knee when they turn or pivot. This instability is particularly problematic when participating in pivoting sports such as soccer and football. The ligament sits just in front of its counterpart, the posterior cruciate ligament, directly in the middle of the knee joint.
Mechanism of Injury
Most anterior cruciate ligament tears occur during a sporting activity and usually in younger patients. When you consider the number of sport hours played, they are more common in women. There have been a variety of reasons proposed for this, such as muscle imbalance and slight variations in the anatomy of the knee joint in women compared to men. The most common sports are football and basketball in younger patients; skiing injuries predominate in older patients. It is, however, possible to injure the anterior cruciate doing a variety of activities. We’ve seen bilateral ACL tears in a weight lifter who was doing an incline bench and popped both his knees at the same time when bench-pressing 350 pounds. It can also be a work-related injury. Interestingly, most people would expect that it is due to contact, but this is not true. Mostly it is a non-contact deceleration where the athlete suddenly turns to the opposite side of the planted and injured knee. As the patient turns and pivots the ligament tears. In basketball it is usually a result of a hyperextension and internal rotation of the tibia on the femur, associated with deceleration.
Usually the patient will feel a sudden pop in their knee immediately in injury to the knee. Surprisingly, sometimes the knee will not get very swollen, although it certainly can. The injury is often missed because the physical examination requires some experience and training. It might actually be easily missed in the initial stages.
Natural History of the Torn Anterior Cruciate Ligament
If left untreated the laxity which is immediately present only becomes worse. The other structures of the knee try in vain to provide some stability to the knee. Over time and with more usage these other structures stretch out as well, resulting in increased instability and then associated meniscal (cartilage) tears. There is an incidence of approximately 1 in 3 patients who at the time of the anterior cruciate ligament tear will tear their cartilage as well. This progresses with time because in an untreated knee the knee is unstable and produces greater stress on the cartilage. Up to 80% of the knees will eventually develop a cartilage tear. The smooth Teflon lining of the knee which is known as articular cartilage is often damaged at the time of the ACL tear. If left untreated, this will again progressively wear at the knee, causing an increased rate of osteoarthritis development. The patients will alter their gait and will develop a rather specific quadriceps avoidance gait because when they contract their quads during normal walking its slides the tibia forward which is usually stopped by the anterior crucial ligament. The patient will naturally and unconsciously try to prevent this. All these problems mean that the knee will progress to late degenerative changes and osteoarthritis much earlier than in a normal knee. There is not good evidence that bracewear alone will decrease the rate of re-injury to the knee. However, in older and non-active patients there is definitely a role for non-operative treatment by simply modifying their activities and avoiding all situations where they may pivot and damage their knee further.
Mechanics
The anterior cruciate is the main factor causing resistance to the anterior displacement of the tibia on the femur. This is demonstrated when the orthopedic surgeon pulls the tibia forward on the femur performing a test of the anterior cruciate ligament. The tibia will displace much further forward than it should when the ACL is torn. The ligament is tight when the knee is in full extension and has the least amount of tension at approximately 45’ of flexion. Because there are different bands to the anterior cruciate ligament different areas of the anterior cruciate tighten at different angles of the knee.
Physical Examination
Examination immediately at the time of injury will reveal usually at least mild swelling of the knee, but not necessarily. The best test is called a Lachman Test where each of the examiner’s hands are placed just above and just below the knee joint. The lower bone is brought forward with the knee angled at approximately 15’ and the examiner assess the end point. Usually, there is a firm endpoint with an intact ACL when the tibia is pulled forward. When the ligament is torn that endpoint is no longer present. The examiner will also look for increased excursion of the tibia forward on the femur. A Drawer Test is when the knee is flexed to 90’. Essentially, the same test is performed. It is more difficult in an acute situation to perform this test because usually the athlete’s knee is too sore to allow the knee to bend to 90’. A Pivot Shift is a test where the knee is brought from an extended position into flexion. Usually the knee will show a slight and subtle shift as the tibia rotates on the femur and shifts back into proper position. It is actually subflexed in the full extended knee position and returns to its natural position as the knee is flexed. As it returns to its natural position there is a “pivot shift” which takes experience to detect.
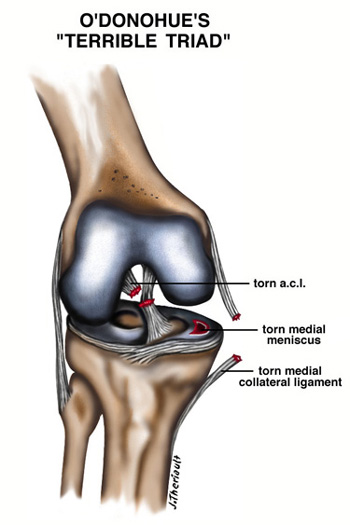
Associated injuries are always assessed for at the same time. Joint line tenderness representing torn cartilage and tenderness over the lateral knee which may reflect tearing of the collateral ligaments. O’Donohue’s “terrible triad” injury involves not only the ACL, but also the medial meniscus and the medial collateral ligament. It is unfortunately fairly common.
Treatment
Originally it was felt that the knee should be repaired surgically as soon as possible. Now, most orthopedic surgeons feel that the swelling should subside and the patient should work to improve range of motion with physiotherapy for 2-3 weeks. Once this is accomplished the patient can then proceed to an anterior cruciate ligament reconstruction. As stated earlier, surgery does not have to be performed on a sedentary older patient, but it is almost always recommended to a younger, active athlete that they should have anterior crucial tear repaired. With modern techniques it is performed as an outpatient – the patient is discharged from the hospital the same day. The patients will leave the hospital on crutches wearing a knee immobilizer for approximately 10 days while they are up and getting around. When the immobilizer comes off, the patient usually will use a passive motion machine that moves the knee through flexion and extension. Physical therapy is started immediately post-operatively. Treatment of a torn anterior crucial ligament in the older patient usually consists of physical therapy and exercise training as well as potentially brace-wear for some activities.
Surgical Treatment Options
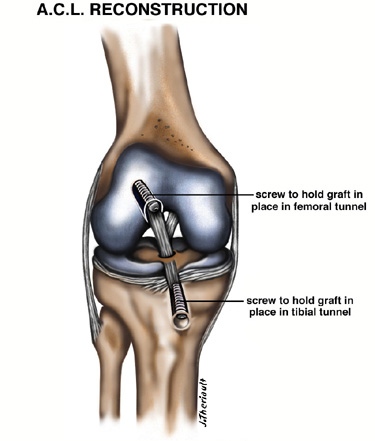
There have been many options described for the surgical treatment of the anterior cruciate ligament. The most popular and currently recognized as the gold standard at this point is an operation where the middle one third of the patella tendon is used as a graft. It is virtually impossible to repair the ligament that is torn. The torn ACL is simply removed and the replaced with the patella tendon graft. Two thirds of the patella tendon is left behind and it will repair itself, not compromising the function of the knee. At each end of the patella tendon a bone block is also taken; one piece from the tibia, and the other from the patella (kneecap). These two bony blocks are inserted into holes that are drilled into the tibia and femur and held into place with screws, which provide stabilization of the ligament graft.
There are other tissues that can be used to substitute for the anterior crucial ligament. Most commonly the second choice are hamstring tendons which are weaved into a graft close to the size of the anterior crucial ligament. We have also used quadriceps tendon and allograft. An allograft is donated cadeaver tissue which is freeze dried until the time of usage upon which time it is thawed out and trimmed to size and used as an ACL substitute. The advantage of an allograft operation is that there is a smaller incision required, the rehab is shorter, and less painful. The disadvantage is that it is not quite as strong as a graft formed from the patient’s own tissue.
Risks, Complications and Alternatives to Surgery
Any time an operation is performed no matter how small or major there are going to be a risks. With anterior cruciate surgery the most common risks are infection, blood clots in the legs, failure of the graft, stiffness of the knee, and persistent pain and instability. There are other rare complications such as neurovascular injury and medical complications both general and related to the anesthetic. All would have to be understood and accepted by the patient prior to the surgery. In particular, all of these should be discussed with your surgeon pre-operatively. Unfortunately, there is no way to perform any surgery without some risks, but the results of anterior cruciate surgery are better than 90-95% effective. Even if a complication does occur it can usually be treated and resolved.
Long Term Prognosis
With an anterior cruciate ligament repair, the patient’s long-term prognosis without any other associated significant injury is excellent. It certainly carries a much better prognosis than when the knee if left untreated. The patient can usually return to any activity that he was doing pre-operatively and many athletes have gone on to excel again at their chosen sport.