
Arthroscopic Knee Surgery
What is it?
Today’s active lifestyle can ask too much of our knees. Athletes often suffer knee injuries from a sudden blow or fall, or simply by twisting. Women are particularly prone to kneecap problems, while older adults may have trouble from aging joints. Many knee problems arise from damage to the soft tissues (the cartilage and ligaments) inside the joint. Until recently, these could not always be easily diagnosed.
 Knee Anatomy
Knee Anatomy
 Knee Anatomy
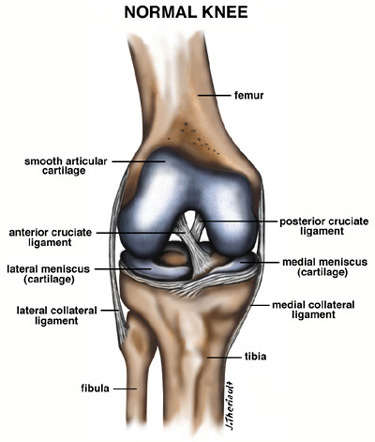
Knee AnatomyThe knee is the largest joint in the body. It is classified as a hinge joint and connects the upper and lower leg bones (femur and tibia). Articular cartilage covers the ends of these bones and the underside of the kneecap (patella). The lateral and medial menisci are cushions of cartilage between the bones. Ligaments and quadriceps give the knee stability and strength.
History/Physical Exam/Diagnostic Tests
Because the knee is vulnerable to soft-tissue and other injuries, orthopedic surgeons see a large number of cases involving the knee. Before treatment, the surgeon must have an accurate diagnosis based on patient history, physical examinations, X-rays, and lab tests (if deemed appropriate). With arthroscopy, the doctor can now look directly into the knee to confirm the diagnosis and, in many cases, surgically correct the problem at the same time.
You will most likely be asked whether the onset of your pain was gradual or from a sudden injury. Your physician will manually examine your knee, looking for tenderness, swelling, a decreased range of motion, and/or instability.
X-Rays
Routine X-rays are commonly used in diagnosing conditions of the bones, while special stress X-rays may be necessary to determine joint stability. Soft tissues cannot be seen, but abnormal bone anatomy and arthritic conditions can often be identified.
Magnetic Resonance Imaging (MRI)
Magnetic Resonance Imaging is a modern technology that can provide information about the soft tissues of the knee (ex: cartilage & ligaments), that ordinary X-rays cannot provide. However, MRI’s are not always 100% accurate.
What is an Arthroscopy?
Arthroscopy is a surgical procedure that allows a physician to treat a damaged or problem knee without making a large incision on the outer skin, which protects the knee joint.
Fiber-optic technology has led to the creation of the arthroscope, an instrument that allows our team to look directly into the knee and diagnose most problems. The arthroscopic shaft contains coated glass fibers and a series of magnifying lenses that beam an intense, cool light to relay a magnified image to the viewer. Looking through the eyepiece or at a television monitor, the surgeon has a clear view and access to most areas of the joint.
Until the advent of the arthroscope, an orthopedic surgeon was unable to directly identify many knee problems. In order to diagnose and treat a problematic knee, the surgeon resorted to conventional open surgery, requiring large incisions, a hospital stay, and often a prolonged recovery. Arthroscopic surgery allows for a direct and thorough examination of the knee. The arthroscope is inserted through tiny incisions called portals. Once the arthroscope is in place, several different instruments may be introduced to treat the affected joint. Forceps, probes, shaving motors, and surgical lasers are some of the most common instruments used in conjunction with the arthroscope. Most problems can be diagnosed accurately and, in many cases, surgically treated at the same time. The whole procedure can usually be performed on an outpatient basis.
Alternatives
Alternatives to arthroscopic knee surgery are anti-inflammatory pills, injections, observation, physical therapy, tolerating the problem, total joint replacement, osteotomies, etc. Alternatives will vary based on age and symptoms.
Common Knee Problems Found at Arthroscopy
 Meniscus Injuries (Cartilage)
Meniscus Injuries (Cartilage)
 Meniscus Injuries (Cartilage)
Meniscus Injuries (Cartilage)Recovery after a meniscus injury depends on how badly the meniscus and other tissues in your knee are damaged. With a mild injury, your recovery may take only 1-2 weeks, or less. With a severe injury, your recovery may take up to 1 month or longer.
Arthroscopic Findings
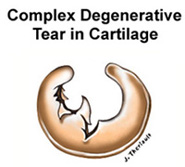
Your meniscus can tear in a variety of ways. With a mild injury, our team may find a small tear along the edge of the meniscus that can simply be trimmed smooth. With a severe injury, the tear is often larger, involving most of the meniscus. With more severe meniscus damage, you may experience more swelling, discomfort, and a longer recovery.
Meniscus Surgery
If you have a mild injury, our team removes the torn flap of cartilage and trims your meniscus back to healthy tissue, leaving a balanced, stable rim. For a more severe injury, your surgeon may need to remove more meniscus, but will leave as much healthy meniscus as possible. After arthroscopy, surface cartilage takes over to absorb shock for the removed meniscus. In some cases, a torn meniscus can be saved by suturing.
|
It is important to know that if your meniscus is repaired, an open incision might be used and you will have a prolonged recovery period with up to six weeks on crutches and up to six months of restricted activities. This procedure can still fail, and require further surgery. |
 Wear & Tear Problems
Wear & Tear Problems
 Wear & Tear Problems
Wear & Tear ProblemsRecovery from a wear and tear problem depends on the extent of surface cartilage damage sustained, and the nature of the surgery performed to fix it. With a mild problem, your recovery may take one to two weeks. With a severe problem, your recovery may take as long as two months, or MAY NOT BE HELPED WITH ARTHROSCOPIC SURGERY ALONE. As you get older, the likelihood of relief with arthroscopy goes down, and should be approached with lower expectations and caution, after other more conservative treatment fails.
Arthroscopic Findings
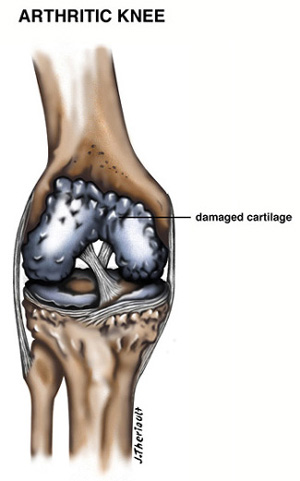
With mild wear and tear, we may find worn or cracked surface cartilage. With severe wear and tear, the surface cartilage may be completely worn through to expose the bones of your knees. Loose bodies of cartilage, bone spurs (excess bone growth), and meniscus damage are also common. (In these severe cases, the arthroscope cannot be expected to relieve symptoms, and further surgery at a later date may be required) The arthroscopic examination, however, helps in the planning and timing of future surgery.
 Surface Cartilage Surgery
Surface Cartilage Surgery
For a mild wear and tear problem, our team may shave and smooth the rough cartilage. For a more severe wear and tear problem with areas of exposed bone, the surgeon uses a special burr to abrade the underlying bone to stimulate new cartilage growth. He may also remove any loose bodies and bone spurs, and trim any damaged meniscus. You may have a biopsy for cartilage growth, which will be performed in a lab.
Patella (kneecap) Problem
(see also Patellar Problems)
Recovery from a patella problem depends on how much patella and surface cartilage damage has been sustained. With a mild problem, your recovery may take only 1-2 weeks. With a severe problem, your recovery may take up to one or two months, or may not be helped with arthroscopic surgery at all, and may require further surgery.
Arthroscopic Findings
You may have pain and tenderness caused by rough surface cartilage under your kneecap, a condition called chondromalacia. Another possibility is that your surgeon may find a misalignment problem (i.e. your patella is not centered correctly in the groove in your thighbone). With misalignment, you may also have chondromalacia, exposed bone surfaces, and loose bodies of cartilage.
Patella Surgery
For chondromalacia, our team can smooth the shaggy surface cartilage under your kneecap. If you also have a misalignment problem, your surgeon can release the bands of dense connective tissue that pull your patella “off center” in a procedure called a lateral release. We may also smooth any rough surface cartilage and worn bone surfaces.
Recovery for All Arthroscopic Surgeries
How quickly and fully you recover after arthroscopy is, to a large degree, up to you. Even if you have only a few tiny incisions, your knee needs special care at home. Elevation and ice can help to control swelling or discomfort, and circulation exercises help prevent post-operative complications. These simple precautions can help keep you comfortable, as well as allow you to start your home recovery exercises as soon as possible.
Elevation reduces swelling, which in turn relieves pain and speeds your healing. Elevation also prevents pooling of blood in your leg. To elevate your knee correctly, be sure to keep your knee and ankle above your heart. The best position is lying down, with pillows lengthwise under your entire leg. Elevate your knee whenever you are not on your feet for the first days after arthroscopy. Ice is a natural anesthetic that helps relieve pain. Ice also controls swelling by slowing the circulation in your knee. To ice your knee, fill a small plastic garbage bag with ice (crushed is best). Wrap the ice bag with a small towel to protect your skin. Completely cover your knee, leaving the ice on for 30 to 60 minutes, several times a day, for the first two or three days after arthroscopy. Avoid hot tubs, Jacuzzi’s, or heating pads unless otherwise advised to.
Pain medication allows you to rest comfortably and start your recovery exercises with minimum discomfort. It is a good idea to take your pain medication at night, even if you are not in severe pain, to assure a good night’s sleep. Pain often signals over-activity, so you might try rest and elevation to help relieve discomfort. Avoid alcohol if you are taking pain medication.
Circulation exercises help prevent post-operative complications such as blood clotting in your leg. Point and flex your foot, and wiggle your toes, every few minutes you are awake for a week or two after arthroscopy. Your dressing keeps your knee clean and helps prevent infection. There will be a bandage over your stitches and a tensor bandage over that. The actual dressing should remain on your knee until you see our team. The knee wrap MUST be taken off at night and then put back on again in the morning.
Showers are fine, after FOUR days. Cover your leg with a plastic garbage bag tied above your dressing. Wait to take your first shower when you can stand comfortably for 10-15 minutes.
Return to work only after our team feels it is safe. It could be a few days or a few weeks, depending on how quickly you heal and how much demand your job puts on your knee. In general, you can count on returning to work sooner after arthroscopic knee surgery than after open knee surgery. Obviously, an office worker at a desk job could go back sooner than a manual laborer.
Home Recovery Exercises
Rebuilding the muscles that support your knee – quadriceps, hamstrings, and calf muscles – is one of the best ways to help your knee recover fully. The sooner you start these exercises, the better. Your goal is to avoid both over-use of these muscles (this causes inflammation, pain, and swelling), and under-use (this causes stiffness and atrophy). You will get the most benefit from these exercises if you do them with slow, steady movements, and on both legs to maintain your muscle balance.
For Strength
Quadriceps sets help rebuild your front thigh muscles, which give your knee its greatest ability. “Quad sets” can be done anywhere, anytime, while lying down or sitting up. Simply tighten your quadriceps, pressing your knee toward the floor or bed. Hold for 5-10 seconds and then relax. It may help to rest your hand on your kneecap and feel it move upward slightly as you tighten your muscles.
Straight leg raises are another exercise that help rebuild all of the muscles that support your knee. Lie on your back and do a “quad set.” Lift your leg 8-12 inches, hold 4-6 seconds, then slowly lower and repeat. When tolerated, add weights or ask a friend to hold your leg down to provide resistance.
Walking also helps you regain range of motion in your ankle, knee, and hip. Even if you are on crutches and not yet bearing full weight on your leg, you can start walking to improve circulation, and speed the healing process in your leg. Try to keep your ankle, knee, and hip bending as normally as possible. Gradually put more weight on your leg, and walk a little farther, as tolerated.
Physical Therapy
After arthroscopic knee surgery, your physician may prescribe therapy for a complete knee rehabilitation program to help you regain your full knee potential. Usually, however, most people do not need formal physiotherapy. As a member of your recovery support team, your physical therapist is a specialist in helping you regain strength and range of motion in your knee. Your physical therapist can design an individualized program for you based on your knee injury and your recovery goals, and can help answer your questions about a safe return to your normal activities. Your program may include knee exercises, special equipment, and other forms of treatment.
Aerobic Exercise
Even before your knee is fully recovered, you can return to a modified exercise program. The safest way to start getting back in shape is with non-weight bearing exercise, such as cycling or swimming. These are excellent forms of aerobic exercise, since they provide steady, continuous conditioning for your heart and lungs. Be sure to check with our team before running or returning to your other favorite fitness activities.
Your Recovery Support Team
Your surgeon, the nursing staff, and if prescribed, your physiotherapist, can coach you towards a safe, speedy recovery after arthroscopic knee surgery. Like an athlete in training, YOU are ultimately in charge of your progress and success. Members of your support team can explain why you need to elevate, ice, and exercise your knee. It is up to you to follow their advice, so you can get back on your feet and safely return to the sports and other activities you enjoy.
Final Facts
- Removal of a small fragment of meniscus does not significantly increase the risk of osteoarthritis later.
- Leaving an unstable fragment of meniscus in a knee, which produces pain and swelling with activity, significantly increases the risk of osteoarthritis.
- Removal of the unstable torn fragment of the meniscus in the bowlegged individual is only part of the solution. Either a correction of the deformity (osteotomy) or total knee replacement may be necessary in the future when the patient is older.
- Removal of a fragment of torn meniscus in the osteoarthritic knee will have a guarded prognosis due to the underlying osteoarthritis.